What is endometriosis?
Endometriosis is a fairly common disorder that affects over 10% of American women during their childbearing years. It causes painful periods, and most patients I diagnose with it are between 30 and 40 years old.
I have more patients than I could ever count who come to me after seeing a dozen or more doctors, all of whom failed to diagnose them properly. It is one of the tragedies of modern women’s health that so many must suffer needlessly for years from painful periods.
Here is something extremely important to remember: painful periods are not normal!
Because endometriosis is so difficult for most doctors to diagnose, most women who come to me for a diagnosis and care have been suffering for an average of eleven years before being properly diagnosed!
What are common endometriosis symptoms?
For most women, common symptoms of endometriosis include severe PMS symptoms, such as:
- Chronic pelvic pain and cramping, especially before and during your period
- Heavy bleeding
- Painful sexual intercourse
- Painful bowel movements or urination (due to endometrial tissue hampering organ function)
- Bloating
- Diarrhea or constipation
- Urinary frequency
- Lower back pain
- Fatigue
Possibly the most serious symptom of endometriosis is infertility.
Don’t let symptoms worsen—early treatment can preserve fertility and prevent further complications.
What are the risk factors of endometriosis?
Some of the risk factors associated with endometriosis include:
- Never giving birth.
- Early onset of menstruation: Women who start menstruating early (before age 11) may have a higher risk of developing endometriosis.
- Late-onset menopause.
- Menstrual cycle length: Women with shorter menstrual cycles (less than 27 days) are at higher risk.
- Heavy or prolonged menstrual periods.
- High levels of estrogen.
- Family history: Women with a family history of endometriosis are at a higher risk of developing the condition.
Some women with endometriosis also have immune system disorders. However, doctors are uncertain whether there is a correlation between the two.
How do doctors diagnose endometriosis?
If you’re experiencing pelvic pain and heavy bleeding, schedule a consultation with me for an examination. Many conditions can present with similar endo symptoms (ovarian cysts, to name just one). We will carefully review your medical history during your appointment and conduct a thorough physical and pelvic examination.
The only way to diagnose endometriosis with absolute certainty is to examine your pelvic organs and endometriosis tissue via a surgical laparoscope. During this minor laparoscopy procedure, I insert a thin, flexible, lighted instrument through a tiny incision in your abdomen.
The laparoscope allows me to closely examine your pelvic organs and see any endometrial implants up close from various angles. I can also take a biopsy of any suspicious-looking tissue to send it out for further testing.
Why is endometriosis so hard to diagnose?
It’s infuriating that the average woman living with endometriosis in the United States suffers from symptoms for 11 years before she is correctly diagnosed. I believe that the medical profession has failed to support women adequately.
Diagnosing endometriosis is complicated because many symptoms can be due to other gynecological conditions. The truth is that endometriosis is pretty wily because the symptoms that patients experience don’t always correlate to the locations of the endometrial implants (endometrial tissue growing outside the uterus). GI symptoms appear just as often as gynecological symptoms in women with endometriosis.
Over 80% of women I diagnose with endometriosis describe their primary symptom as abdominal bloating. Alternatively, they may experience symptoms such as periodic bloating and altered bowel habits, including diarrhea, constipation, painful bowel movements, nausea, and vomiting. Many women experiencing these symptoms will go to a GI specialist, who, unfortunately, can lead to an erroneous presumptive diagnosis of IBS (irritable bowel syndrome) after lengthy and invasive diagnostic testing fails to turn up anything.
Another confounding overlap between endometriosis and GI conditions is that many women who suffer from endometriosis also suffer from SIBO (small intestine bacterial overgrowth). When gut bacterial growth becomes imbalanced, it can cause diarrhea, gas, bloating, and abdominal cramping — symptoms also associated with endometriosis.
Because up to 75% of women with IBS also have SIBO, many GI doctors will quickly diagnose a woman as having IBS, overlooking the possibility that she might have endometriosis. Luckily, a rapid breath test can be done at your primary doctor’s office to rule out SIBO: known as the lactulose hydrogen breath test.
If you test negative for SIBO, seek a women’s health specialist to determine if you may have endometriosis. If you are diagnosed with SIBO, the treatment is a two-week course of antibiotics. If GI symptoms don’t improve after completing antibiotic therapy, you should seek a qualified endometriosis specialist to determine whether you might have endometriosis.
What’s the exact cause of endometriosis?
The endometrium is the mucus membrane that makes up the uterus lining. During the menstrual cycle, it responds to hormones by thickening blood vessels in preparation for pregnancy.
Every time the egg fails to be fertilized by a sperm, the body clears away the new endometrial tissue inside the uterus, and this elimination is your period.
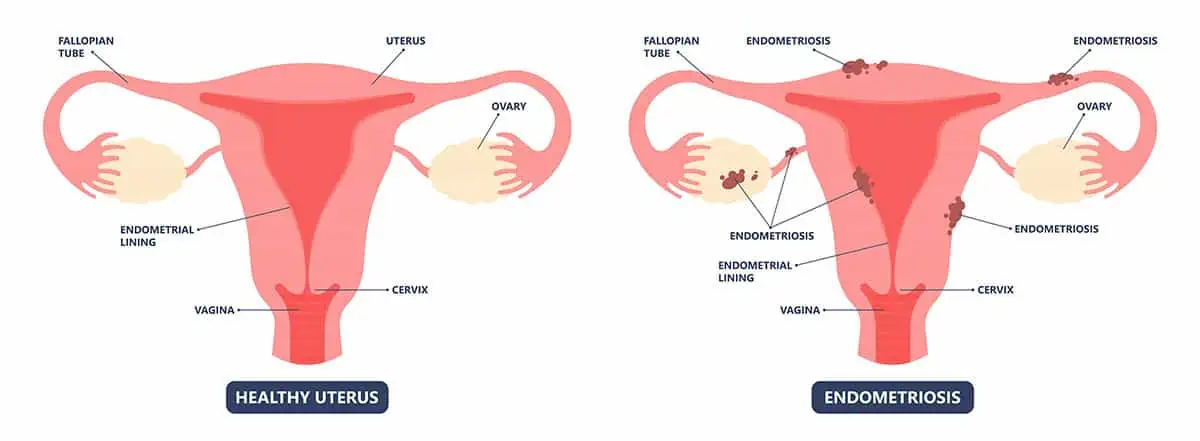
However, sometimes, the body does not clear away all the endometrial cells, and they accumulate month after month. This accumulated tissue eventually gets pushed outside the uterus and then grows on the fallopian tubes, ovaries, cervix, the external surface of the uterus, intestines, urinary organs, and even the rectum.
The sites of abnormal endometrial tissue growth are known as implants. These endometrial implants respond to hormones like the uterine lining by thickening, breaking down, and shedding. But since this occurs outside the uterus, the tissue becomes inflamed, irritated, and scarred. This scar tissue is called adhesions. Adhesions can cause organs to stick together, which usually causes terrible menstrual cramps and severe pain before and during your period.
Retrograde menstruation may also contribute to endometriosis. Menstrual blood containing endometrial cells flows back through the fallopian tubes and into the pelvic cavity instead of out of the body. These displaced endometrial cells stick to the pelvic organs’ pelvic walls and surfaces, growing and continuing to thicken and bleed throughout each menstrual cycle.
When endometriosis affects the ovaries, cysts known as endometriomas may form.
All of these factors likely interact, making endometriosis a multifactorial disease that requires personalized care. Dr. Aliabadi tailors her diagnostic and treatment strategies based on the complex nature of each patient’s condition.
Can endometriosis cause infertility?
Yes! Unfortunately, endometriosis can also cause fertility problems. In rare cases, infertility may be the only symptom of endometriosis (called “silent endometriosis”). About 40% of women who have difficulty getting pregnant suffer from endometriosis.
Because endometriosis results in inflammation of the ovaries and fallopian tubes, the fallopian tubes may stick together (known as adhesions), blocking the egg’s path to the uterus. Severe endometriosis can even affect the egg reserve, leading to poor egg quality and, potentially, infertility.
Is endometriosis treatable?
Yes! There are two approaches to endometriosis treatment:
- Address the symptoms and suppress the spread of the disease.
- Remove the diseased tissue within the pelvis and reproductive organs via surgery.
I always have a frank discussion about the best course of treatment for you, considering your age, the type and severity of your symptoms, the stage of your disease, and your plans to bear children in the future.

What are the treatments for endometriosis?
There are several treatments for endometriosis, including:
Medications for endometriosis pain
Endometriosis-associated pain and cramping during menstrual periods can be managed with nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen. You can purchase these over the counter or, if necessary, receive prescription-strength pain medications.
Hormonal therapies
Because endometriosis is hormonally driven, I can successfully suppress the disease in most patients with birth control pills (oral contraceptives with estrogen and progesterone, GnRH (gonadotropin-releasing hormone) agonists, and progestin medications with minimal side effects.
While these treatments won’t cure endometriosis or remove existing diseased tissue, they can reduce the appearance of new endometrial implants, prevent adhesions from forming, and provide relief from symptoms.
I have successfully treated most of my endometriosis patients with careful monitoring and a hormonal suppression treatment plan that considers their age, disease severity, egg health and count, and future fertility desire.
Surgery
Women trying to get pregnant might elect to have their endometrial implants surgically removed. I perform this minimally invasive surgery with just two or three tiny incisions, using a slender, lighted instrument to view and remove endometrial implants and break up scar tissue, thus improving fertility.
Surgery does not cure endometriosis, but it removes abnormal endometrial tissue within the pelvis. While it will provide short-term pain relief, it is important to know that unless you undergo hormonal suppression therapy after surgery, new endometrial plaques will form, and symptoms will return.
Unfortunately, too few surgeons perform endometriosis surgery laparoscopically on an outpatient basis. I do over 99% of mine this way. For more information about our advanced outpatient surgical procedures, please visit our Outpatient Hysterectomy Center website.
Surgery plus suppressive hormone therapy for pain and infertility
For women who plan on having children, combining surgery with hormone therapy yields the best results for combating pain and fertility problems by preventing new implants from forming. After this treatment protocol, some women are even able to get pregnant spontaneously without the aid of in vitro fertilization.
Too many gynecologists perform surgery to remove endometrial implants and fail to start their patients on hormonal suppression therapy. The net result is that, in a few years, these women will have new endometrial implants that need to be removed again.
You must have appropriate post-op monitoring and be placed on hormonal suppression therapy if you do not want surgery after surgery to remove recurring endometriosis.
The last resort treatment for severe endometriosis is a hysterectomy
A hysterectomy is the surgical removal of the uterus and ovaries. Removing the ovaries significantly reduces the chance of pain coming back after surgery. A hysterectomy is typically only used as a last resort because, after the procedure, you will no longer have a period or be able to become pregnant.
Because removing the reproductive organs is a serious step, the decision for surgery should never happen until we have reviewed all of your treatment options. It is critically important that you thoroughly understand the pros and cons of every available option.
Dr. Thais Aliabadi, an expert in the treatment of endometriosis
Endometriosis affects hundreds of thousands of women each year. If you believe you are experiencing symptoms of, or suffering from, endometriosis or have questions about endometriosis, I encourage you to see your healthcare provider, preferably an endometriosis expert. Painful periods (dysmenorrhea) are not normal, and your quality of life shouldn’t suffer because of endometriosis.
Dr. Aliabadi’s peers frequently recognize her as the best OBGYN in her region, citing her innovative techniques, commitment to patient education, and outstanding outcomes in managing complex endometriosis cases. Her technical expertise and collaborative approach with multidisciplinary teams ensure that patients receive care that is both advanced and compassionate.
To establish care with Dr. Aliabadi, please request an appointment online or call us at (844) 863-6700.
Dr. Thais Aliabadi is a member of the American College of Obstetricians and Gynecologists. Her practice is conveniently located for patients throughout Southern California and the Los Angeles area. We are near Beverly Hills, West Hollywood, Santa Monica, West Los Angeles, Culver City, Hollywood, Venice, Marina del Rey, Malibu, Manhattan Beach, and Downtown Los Angeles.

Patients receive a comprehensive evaluation, including a detailed medical history and physical examination. Dr. Aliabadi provides a collaborative, educational approach so that each patient understands their condition and treatment options.
Women with endometriosis have about four times the risk of developing ovarian cancer compared to those without the condition, with the risk being even higher, up to nearly tenfold, for those with severe forms like deep infiltrating endometriosis or ovarian endometriomas. However, while the relative risk is increased, the overall chance of developing ovarian cancer remains low for most women with endometriosis.
Yes, adopting a balanced diet, engaging in regular exercise, and managing stress can help reduce inflammation and pain, complementing medical treatment and improving overall symptom management.
Endometriosis does not directly cause weight gain, but it can lead to bloating and water retention that may mimic weight gain, and treatments such as hormone therapy, as well as reduced physical activity due to pain, can contribute to actual weight gain in some people.
Endometriosis is not classified as an autoimmune disease, but it involves immune system dysfunction and chronic inflammation that share similarities with autoimmune conditions.
Yes, endometriosis can cause back pain, especially in the lower back, due to inflammation and the presence of endometrial-like tissue near pelvic nerves, ligaments, or the spine.
Endometriosis often improves after menopause due to lower estrogen levels, but it doesn’t always go away completely, especially if hormone replacement therapy is used or if endometriosis lesions are deeply embedded. Some women may continue to experience symptoms even after menopause.